England: Brain Cancer Incidence Increased in Temporal and Frontal Lobes of Brain since 1995
A new study of cancer data in England essentially replicated the results of the Philips et al study (see below). The study found that the two age groups most vulnerable to carcinogenic effects from cell phone use — young and elderly adults — showed increased incidence over time in brain cancer in the frontal and temporal lobes of the brain — the two lobes that receive the greatest dose of microwave radiation when cell phones are used near the head during phone calls.
However, Frank de Vocht, the author of this paper, rejected the explanation that cell phone use caused the increased cancer risk. He attributed the increased incidence to better diagnosis of brain tumors, especially in the elderly. Of course, this does not explain why the increase was only observed in the frontal and temporal lobes. He did not rule out the possibility that cell phone radiation may be a contributing factor to the observed increase.
Microwave News reported on this study and published the following graph obtained from Alasdair Philips (Microwave News, “Location, Location, Location: Aggressive Brain Tumors Tell a Story; GBM Rise Only in Frontal and Temporal Lobes, Oct 26, 2018.)

de Vocht F. Analyses of temporal and spatial patterns of Glioblastoma Multiforme and other brain cancers subtypes in relation to mobile phones using synthetic counterfactuals. Environmental Research. Available online 17 October 2018. https://doi.org/10.1016/j.
• English 1985–2005 brain cancer subtype rates were compared to counterfactual trends
• Excess GBM increases were found in the frontal and temporal lobes, and cerebellum
• Mobile phone use was unlikely to have been an important putative factor
• No evidence of an effect of mobile phone use on acoustic neuroma and meningioma
Abstract
This study assesses whether temporal trends in glioblastoma multiforme (GBM) in different brain regions, and of different malignant and benign (including acoustic neuroma and meningioma) subtypes in the temporal lobe, could be associated with mobile phone use.
Increases in excess of the counterfactuals for GBM were found in the temporal (+38% [95% Credible Interval -7%,78%]) and frontal (+36% [-8%,77%]) lobes, which were in agreement with hypothesised temporal and spatial mechanisms of mobile phone usage, and cerebellum (+59% [-0%,120%]). However, effects were primarily present in older age groups, with largest effects in 75+ and 85+ groups, indicating mobile phone use is unlikely to have been an important putative factor. There was no evidence of an effect of mobile phone use on incidence of acoustic neuroma and meningioma.
Although 1985–2014 trends in GBM in the temporal and frontal lobes, and probably cerebellum, seem consistent with mobile phone use as an important putative factor, age-group specific analyses indicate that it is unlikely that this correlation is causal.
Excerpts
Assessment of specific cancer subtypes in the temporal lobe indicated that the excess incidence was mainly found for GBM, with similar trends observed in the frontal lobe and cerebellum…. The increased rates of specific brain cancer subtypes in excess of the counterfactuals correspond to the spatial and temporal patterns that would be expected if exposure to RF from mobile phones were an important putative factor (Cardis et al., 2008, Morgan et al., 2016) … However, age group-specific analyses indicate that the excess relative impacts increased with age over 65 years and were primarily found in the very old (75/85+ years of age) for whom it is unlikely that mobile phone use had been an important causal factor. In addition, excess numbers of newly diagnosed cases were also observed in the young (<24 years of age) for whom mobile phone use is also an unlikely causal factor….
The assumption that a 10-year lag was the most plausible period between first exposure and when increased risk could be observed in registry data was based on the previous analyses (De Vocht (2016)). Although sensitivity analysis using a 15-year lag showed no evidence of excesses relative to counterfactuals, this may still have been too short….
Mar 25, 2018
Brain Cancer Increased from 1995 to 2014
from 1995 to 2014 found that the trends over time varied by type of cancer,
especially in the frontal and temporal lobes.
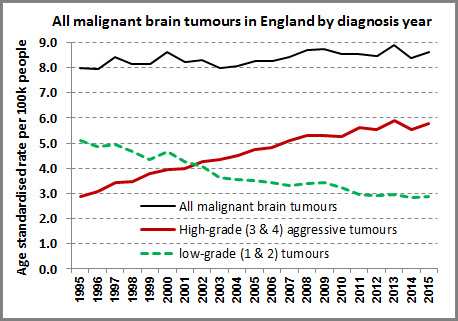
highly statistically significant” increase in glioblastoma multiforme (GBM), the
most common brain cancer, across all ages. The rate of GBM more than doubled
from 2.4 to 5.0 per 100,000 people. However, this increase was mostly hidden
because the overall malignant brain tumor trend was relatively flat due to a
reduced incidence of lower grade brain tumors.
brain accounted for 41% of malignant brain tumors. By 2015, these two sites accounted for 60% of the tumors.
caused these differential trends in brain cancer. Based upon epidemiologic
research, the most compelling explanation for the increased incidence in these
deadly brain tumors, especially in the frontal and temporal lobes, may be
exposure to microwave radiation due to widespread adoption of cell phones. However,
the increased use of CT imaging scans is an alternative, but less compelling,
explanation because far fewer people would have been exposed to this form of
ionizing radiation.
flat-line trend in overall brain
tumor incidence and argue that cell phone use doesn’t cause brain cancer need
to examine data on the location and type of brain tumors over time.
 |
| Source: Alasdair Philips via Microwave News. |
Multiforme incidence in England 1995–2015 suggests an adverse environmental or
lifestyle factor
Philips, Denis L. Henshaw, Graham Lamburn, and Michael O’Carroll. Brain
tumours: rise in Glioblastoma Multiforme incidence in England 1995–2015
suggests an adverse environmental or lifestyle factor. Journal of Environmental
and Public Health. Article ID 7910754, https://doi.org/10.1155/2018/7910754. 2018.
incidence of brain tumour types
recognised quality source
information
incidence time trend
into causal mechanisms
malignant brain tumour incidence over a recent time period.
data covering 81,135 ICD10 C71 brain tumours diagnosed in England (1995–2015)
were used to calculate incidence rates (ASR) per 100k person–years,
age–standardised to the European Standard Population (ESP–2013).
statistically significant ASR rise in glioblastoma multiforme (GBM) across all
ages. The ASR for GBM more than doubled from 2.4 to 5.0, with annual case
numbers rising from 983 to 2531. Overall, this rise is mostly hidden in the
overall data by a reduced incidence of lower grade tumours.
resources and brain tumour aetiology. The rise cannot be fully accounted for by
promotion of lower–grade tumours, random chance or improvement in diagnostic
techniques as it affects specific areas of the brain and only one type of brain
tumour. Despite the large variation in case numbers by age, the percentage rise
is similar across the age groups which suggests widespread environmental or
lifestyle factors may be responsible.
significant increase in primary GBM tumours over 21 years from 1995–2015, especially in frontal and temporal
lobes of the brain. This has aetiological and resource implications.
years of age, the age–standardised AAPC rise is strongly statistically significant in all our
three main analysis age groups.
fully accounted for by improved diagnosis as it affects specific areas of the
brain and just one type of brain tumour which is generally fatal. We suggest
that widespread environmental or lifestyle factors may be responsible.
research into the initiation and promotion of GBM tumours. This should include
the use of CT imaging for diagnosis and also modern lifestyle factors that may
affect tumour metabolism.


https://www.saferemr.com/2018/03/brain-tumor-incidence-trends.html